
Cervical Instability: Causes, Symptoms, & Treatments
Exploring the Unique Causes of Headaches in Denver and How Chiropractic Care Provides Relief
Cervical instability is a medical condition in which loose ligaments between the upper cervical spine and the base of the skull may lead to neuronal damage.
Full disclosure from my years of experience treating patients with chiropractic care: This condition is massively over-diagnosed. However, I consider it with people suspicious of hyper mobility issues or with headaches and disequilibrium issues.
When I suspect cervical instability in a patient, I take a lateral flexion anterior to posterior open mouth x-ray — that’s the best way to visualize it.
If you have cervical instability, you may experience migraines, vertigo, or nausea, among other adverse symptoms. Fortunately, this condition is treatable.
Let’s talk about the symptoms, causes, treatments, diagnosis, and prevention of cervical instability.
What Is Cervical Instability?
Cervical instability occurs when the ligaments in between your spinal cord and skull are loose. These “lax ligaments” allow for excessive movement of the top two cervical vertebrae, which may result in many symptoms, such as headaches, fainting, or even memory loss.
Ligament laxity is a state in which ligaments that attach bone to bone are loose. Also called ligamentous laxity, this condition often causes chronic pain. It can affect the whole body, or only specific parts.
You may have seen a friend hyperextend their finger, seemingly unnaturally. This is probably due to ligament laxity causing joint hypermobility syndrome. The ligaments connecting the bones in your friend’s finger are loose and allow for more range of motion.
This abnormal range of motion in your neck area can trigger cervical instability.
Ligament laxity may be caused by genetic connective tissue disorders, such as Ehlers-Danlos Syndrome or Marfan Syndrome.
There are 2 joints at which the ligaments may be loose, leading to cervical instability:
- Atlanto-occipital joint
- Atlanto-axial joint
Cervical instability is related to:
- Craniocervical instability
- Craniovertebral instability
- Clinical instability of the cervical spine
- Cervical neck instability
- Cervical spine instability
- Atlantoaxial instability
What’s the difference between craniocervical instability and cervical instability?
Craniocervical instability (CCI) and cervical instability are related concepts, but they refer to distinct conditions involving different parts of the spine and skull.
Craniocervical instability involves the junction between the base of the skull (the occiput) and the top of the cervical spine (the first cervical vertebra, C1, also known as the atlas).
Cervical instability involves the cervical spine, which is the neck region of the spine. It involves the vertebrae and ligaments and can affect the spinal cord and nerve roots in the neck area.
Cervical Instability Symptoms
Symptoms of cervical instability often include pain, weakness, numbness, and tingling. More severe neurological deficits may also present such as difficulty with coordination or loss of bladder or bowel control. Other cervical instability symptoms that may occur include:
- Feeling that your skull may “fall off” the spine
- Occipital headaches
- Migraines
- Muscle spasms
- Neck, shoulder , or jaw pain
- Difficulty swallowing
- Tenderness at the base of thee skull
- Light sensitivity
- Blurred vision
- Tinnitus (ringing in the ears)
- Orthostatic intolerance
- Tremors
- Vertigo
- Dizziness
- Clumsiness
- Fainting
- Limb weakness
- Shortness of breath
- Nausea
- Fatigue
- Lhermitte’s sign
- Cognitive decline
- Memory loss
- Loss of bladder or bowel control
- Trigeminal Neuralgia
Cervical spine instability may lead to compression of the spinal cord or nerve roots in the cervical region. This compression can affect the function of the spinal cord, which is an extension of the brain stem.
Abnormal pressure exerted on the nervous system may lead to a variety of neurological symptoms and impairments.
Timely diagnosis and appropriate management are crucial to mitigate the impact on the nervous system and prevent further complications.
Diagnosing Cervical Instability
Diagnosing cervical spine instability can pose a challenge, often requiring the insights of a skilled orthopedic specialist to accurately detect. I can typically spot this problem in patients, but may refer them to an orthopedist to accurately diagnose if that can help open more treatment modality options.
How do you test cervical instability ? The 4 methods for testing cervical instability include:
- Upright MRI: Magnetic resonance imaging
- Supine MRI: Laying on your back
- CT scan : Computerized tomography
- Digital motion x-ray
As I stated earlier, I’ve found that a lateral flexion anterior to posterior open mouth x-ray is the most accurate diagnostic tool for proper visualization of this issue (if it exists).
Abnormalities in the following measurements indicate cervical instability:
- Clivo-Axial Angle: Less than or equal to 135 degrees
- Grabb-Oakes measurement: Greater than or equal to 9 mm
- Harris measurement: Greater than 12mm
- Spinal subluxation : Any amount
MRIs are the most common diagnostic testing method for cervical instability. A 2012 scientific investigation found that MRIs had limited diagnostic value in patients with whiplash-associated disorders such as cervical instability.
Causes of Cervical Instability
Cervical instability is caused by anterior and posterior ligament laxity between the skull and the top two vertebrae (the atlas and the axis ). This allows excessive movement and leads to a long list of physical and neurological symptoms.
Causes of cervical instability may include:
- Whiplash or other injury causing rapid flexion/extension (such as from a car accident)
- Tethered cord syndrome
- Genetics
- Connective tissue disorders (such as Ehlers-Danlos Syndrome or rheumatoid arthritis)
- Chiari malformation
- Degeneration
Treatments for Cervical Instability
There are 5 standard treatments for fixing cervical instability:
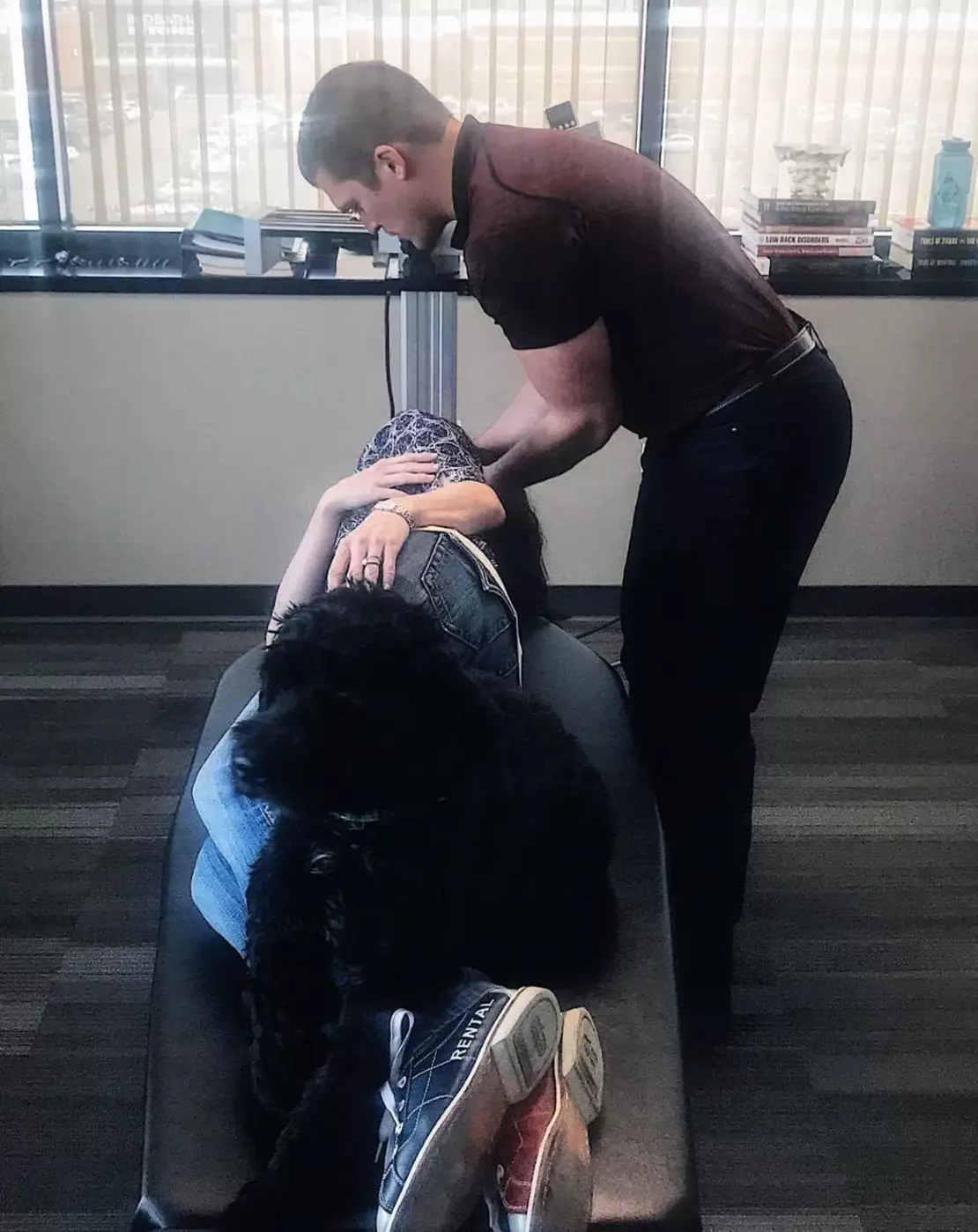
Chiropractic care is a common and effective treatment for headaches , poor posture, and spinal misalignments — all of which are connected to cervical instability.
Upper cervical chiropractic care may correct cervical instability.
This 2020 study demonstrated how spinal chiropractic manipulative therapy can be used to correct cervical instability, joint disorders, dislocations of cervical vertebrae, and much more.
Spinal manipulation is a safe and effective therapy when performed by a highly qualified chiropractor, even in special needs patients. Chiropractic treatment should always be considered before you move on to surgery.
Note: Non-surgical spinal decompression therapy is not recommended for patients with cervical instability.
Gentle adjustments of the upper spine are critical to recovering from cervical instability . Denver, CO residents can receive treatment with us at Denver Upper Cervical Chiropractic . Call us at 303-955-8270 to schedule an appointment.
Does cervical instability require surgery? You do not need surgery for cervical instability unless your instability has gotten out of control. In the most severe cases, surgery may be necessary to manage the severe symptoms of advanced cervical instability.
Most surgical treatments aim to correct dysfunction of the craniocervical junction, where the skull (occiput) meets the upper spine.
The most common surgical treatment options include:
Cervical spine fusion, in particular, may be performed when slight subluxations are detected but before migration of the odontoid to prevent the progression of cervical instability.
Medscape explains that when it comes to surgery for cervical instability, optimal results have been obtained in patients with severe pain and mild myelopathy.
However, more conservative treatments for cervical instability, such as chiropractic care or physical therapy, may also be effective. Since surgery is invasive and expensive, it may be wise to consider more conservative treatments with a healthcare professional.


Physical therapy is a very effective treatment option for cervical instability that strengthens neck muscles and improves stability. We often recommend patients do PT alongside chiropractic care for the best recover outcomes.
What does physical therapy for cervical instability involve?
- Strengthening exercises
- Posture education
- Joint mobilization ( Click here to watch a video of what joint mobilization will look like.)
- Soft tissue mobilization
- Spinal manipulation
- Proprioception exercises
You may or may not need to wear a brace or cervical collar, depending on the severity of your cervical instability, and whether you had surgery beforehand.
According to a two-year follow up study , surgery improved patient outcomes better after one year. But physical therapy was insignificantly different from surgery at improving symptoms after two years.
In other words, surgery is a short-term strategy to offer immediate back pain relief. Physical therapy improves symptoms in the long-term.
Always consult your doctor or physical therapist before trying these strengthening exercises to help with cervical instability.
5 strengthening exercises that may treat or prevent cervical instability are:
- Chin tucks: Chin tucks stretch and strengthen your posture and neck joints. Chin tucks are the most common strengthening exercise used to improve cervical instability.
- Isometric exercises: Isometric exercises can be combined with active range of motion to strengthen the neck area. Click here for a video demonstration by a physical therapist.
- Gentle neck rotation: Rotating the neck slowly and methodically also strengthens the joints and muscles around the upper cervical spine.
- “Yes and no” neck motions: Yes and no neck motions help stretch the muscles and joints around the neck. A yes motion is nodding your head up and down, slowly. A no motion is shaking your head left and right, slowly.
- Good posture: Good posture reduces pressure put on the spine. Practice good posture for as long as you can each day. You should be able to comfortably exercise good posture for longer and longer with each passing day.
Discontinue any exercise or movement that triggers pain. Feeling pain is a sign you should rest and not push yourself further.
Prolotherapy is a relatively new treatment option for patients with cervical instability, often with no adverse side effects.
Prolotherapy is a regenerative injection technique that aims to stimulate the body’s natural healing processes to strengthen and repair injured joints and ligaments.
It is intended for acute and chronic musculoskeletal injuries, including those causing chronic neck pain related to underlying joint instability and ligament laxity, such as cervical instability.
A 2007 case series showed that prolotherapy consistently improved neck pain in whiplash patients.
Stem cell prolotherapy is also a burgeoning treatment for ligament repair.
Prolotherapy injections offer cervical instability patients an alternative to surgery.
Prolotherapy has yet to prove if it can offer repeatable treatment results. Many patients seek out a combination of chiropractic and physical therapy after prolotherapy fails to provide lasting relief.
What is the best treatment for cervical instability ? There is no consensus on the best cervical instability treatment as each case is unique. However, a combination of chiropractic, physical therapy, and strengthening exercises offers the most lasting results.
Pain Management
In combination with the treatments listed above, managing the pain associated with cervical spine instability may involve:
- Medications: Non-steroidal anti-inflammatory drugs (NSAIDs), muscle relaxants, and pain relievers may be prescribed to alleviate pain and inflammation.
- Bracing: In some cases, wearing a cervical collar or brace can provide support and reduce strain on the unstable area.
- Heat and cold therapy: Applying heat or cold packs to the affected area can provide temporary relief from pain and muscle tension.
- Epidural steroid injections: In more severe cases, injections of corticosteroids into the affected area can help reduce inflammation and pain.
It’s essential for individuals with cervical spine instability to consult with a spine specialist, who can assess their specific condition and recommend a personalized treatment plan.
How to Prevent Cervical Instability
Cervical instability is common in people with connective tissue disorders. Individuals at a higher risk, like with Ehlers-Danlos syndrome, will need to actively prevent cervical instability.
To prevent cervical instability:
- Regularly visit your chiropractor
- Do chin tucks for one minute, every day
- Practice good posture every day
- Avoid situations associated with whiplash or other trauma to the spine
Everyone should follow these tips for good overall health, but particularly individuals with connective tissue disorders or malformations of the neck or spine.
Prognosis & Long-Term Outlook
Cervical instability is somewhat rare, but it is likely underdiagnosed. For example, connective tissue disorders that can trigger cervical instability affect at least 1 in 5,000 people worldwide.
If you are experiencing any symptoms of cervical instability, contact your doctor or chiropractor right away.
Can I recover from cervical instability? It is possible to recover from cervical instability by improving the biomechanics of the upper cervical spine. Lasting recovery will require high-quality treatment, such as physical therapy or chiropractic adjustments.
If you’re a Denver, CO resident, schedule an appointment with Denver Upper Cervical Chiropractic. Here, we empower patients to take part in their whole person healing, and we want to help YOU with your cervical instability.
Sources:
- Tominaga, Y., Maak, T. G., Ivancic, P. C., Panjabi, M. M., & Cunningham, B. W. (2006). Head-turned rear impact causing dynamic cervical intervertebral foramen narrowing: implications for ganglion and nerve root injury. Journal of neurosurgery: Spine, 4 (5), 380-387. Full text: http://www.danmurphydc.com/wordpress/wp-content/uploads/archive/2006/Article_22-06.tominaga.pdf
- Lummel, N., Bitterling, H., Kloetzer, A., Zeif, C., Brückmann, H., & Linn, J. (2012). Value of “functional” magnetic resonance imaging in the diagnosis of ligamentous affection at the craniovertebral junction. European Journal of Radiology, 81 (11), 3435-3440. Abstract: https://pubmed.ncbi.nlm.nih.gov/22762971/
- Rebbeck, T., & Liebert, A. (2014). Clinical management of craniovertebral instability after whiplash, when guidelines should be adapted: A case report. Manual therapy, 19 (6), 618-621. Abstract: https://pubmed.ncbi.nlm.nih.gov/24560490/
- Fan, S. T. (2018). Clinical observation on cervical chiropractic for cervical spondylosis of vertebral artery type. Journal of Acupuncture and Tuina Science, 16 (2), 115-119. Abstract: https://link.springer.com/article/10.1007/s11726-018-1034-2
- Wang, Y., Xu, M., & Shi, Y. (2020). Efficacy of spinal chiropractic manipulative therapy for adjusting the relationship between cervical facet joints to treat headache caused by acute mountain sickness. Journal of International Medical Research, 48 (1), 0300060519898005. Full text: https://journals.sagepub.com/doi/full/10.1177/0300060519898005
- Dyck, V. G. (1981). Upper cervical instability in Down’s syndrome: a case report. The Journal of the Canadian Chiropractic Association, 25 (2), 67. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2484266/
- Agarwal, A. K., Peppelman, W. C., Kraus, D. R., Pollock, B. H., Stolzer, B. L., Eisenbeis, C. H., & Donaldson, W. F. (1992). Recurrence of cervical spine instability in rheumatoid arthritis following previous fusion: can disease progression be prevented by early surgery?. Journal of rheumatology, 19 (9), 1364-1370. Abstract: https://pubmed.ncbi.nlm.nih.gov/1433002/
- Maniker, A. H., Schulger, M., & Duran, H. L. (1995). Halifax clamps: efficacy and complications in posterior cervical stabilization. Surgical neurology, 43 (2), 140-146. Abstract: https://pubmed.ncbi.nlm.nih.gov/7892658/
- Yuan, B., Zhou, S., Chen, X., Wang, Z., Liu, W., & Jia, L. (2017). Gallie technique versus atlantoaxial screw-rod constructs in the treatment of atlantoaxial sagittal instability: a retrospective study of 49 patients. Journal of Orthopaedic Surgery and Research, 12 (1), 105. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5504836/
- Huang, K. Y., Lin, R. M., & Fang, J. J. (2016). A novel method of C1–C2 transarticular screw insertion for symptomatic atlantoaxial instability using a customized guiding block: A case report and a technical note. Medicine, 95 (43). Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5089091/
- Chang, H., Park, J. B., Choi, B. W., Kang, J. W., & Chun, Y. S. (2019). Posterior Sublaminar Wiring and/or Transarticular Screw Fixation for Reducible Atlantoaxial Instability Secondary to Symptomatic Os Odontoideum: A Neglected Technique?. Asian spine journal, 13 (2), 233. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6454275/
- Young, B. A., & Ross, M. D. (2009). Neck pain and headaches in a patient after a fall. Journal of Orthopaedic & Sports Physical Therapy, 39 (5), 418-418. Full text: https://www.jospt.org/doi/full/10.2519/jospt.2009.0405
- Engquist, M., Löfgren, H., Öberg, B., Holtz, A., Peolsson, A., Söderlund, A., … & Lind, B. (2013). Surgery versus nonsurgical treatment of cervical radiculopathy: a prospective, randomized study comparing surgery plus physiotherapy with physiotherapy alone with a 2-year follow-up. Spine, 38 (20), 1715-1722. Full text: https://www.diva-portal.org/smash/get/diva2:656650/FULLTEXT01.pdf
- Steilen, D., Hauser, R., Woldin, B., & Sawyer, S. (2014). Chronic neck pain: making the connection between capsular ligament laxity and cervical instability. The open orthopaedics journal, 8 , 326. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4200875/
- Hauser, R. A., Steilen, D., & Gordin, K. (2015). The Biology of Prolotherapy and Its Application in Clinical Cervical Spine Instability and Chronic Neck Pain: A Retrospective Study. European Journal of Preventive Medicine, 3 (4), 85-102. Full text: https://www.researchgate.net/profile/Ross_Hauser2/publication/281131818_The_Biology_of_Prolotherapy_and_Its_Application_in_Clinical_Cervical_Spine_Instability_and_Chronic_Neck_Pain_A_Retrospective_Study/links/57b46ab708ae19a365fae7b3.pdf
- Hooper, R. A., Frizzell, J. B., & Faris, P. (2007). Case Series on Chronic Whiplash-Related Neck Pain Treated with Intra-articular Zygapophysial Joint Regeneration Injection Therapy. Pain Physician, 10 (2), 313. Full text: https://stemcellarts.com/wp-content/uploads/2013/03/Prolotherapy-NeckPain-Chronic-Whiplash.pdf
- Alderman, D., Alexander, R. W., Harris, G. R., & Astourian, P. C. (2011). Stem cell prolotherapy in regenerative medicine: background, theory and protocols. J Prolother, 3 (3), 689-708. Full text: http://journalofprolotherapy.com/stem-cell-prolotherapy-in-regenerative-medicine-background-theory-and-protocols/
- Centeno, C. J., Elliott, J., Elkins, W. L., & Freeman, M. (2005). Fluoroscopically guided cervical prolotherapy for instability with blinded pre and post radiographic reading. Pain Physician, 8 (1), 67-72. Full text: https://www.painphysicianjournal.com/current/pdf?article=Njg%3D&journal=22
The post Cervical Instability: Causes, Symptoms, & Treatments appeared first on Denver Upper Cervical Chiropractic.
© 2026 Denver Upper Cervical Chiropractic